
Measuring Trauma
May 22, 2023Q. Why is trauma such a big issue for adopters?
A. Because our children have unresolved trauma which is like an infected wound.
Q. Why doesn't it just form a scab and scar, now that they are safe?
A. Because infected wounds won't heal if they are constantly touched and poked, they tend to get worse.
Q. How are the wounds being touched?
A. By everyday experiences and sensory triggers.
It took me years to realise that the wounds my children suffered during infancy had not healed, despite me being a really good Mum who was doing many of the right things (and inadvertently a few of the wrong).
I wasn't factoring in trauma enough.
What is trauma and how does it feel?
Trauma can be defined as a "physical or psychological wound or hurt". For infants this includes emotional, physical, psychological and sexual abuse, neglect, frequent changes of primary carer, pain etc. A very dry description.
What does trauma look, sound and feel like to a child? The neglect, the constant changes, the uncertainty, the fear in which they lived - how is that experienced?
- The fear of another move, the pain of staying.
- The fear of seeing birth Mum and the terror of not seeing her.
- The anguish of hello and the grief of goodbye.
- The distress of hunger and confusion of a “Happy Meal”.
- The torment of teasing and the agony of being ignored.
- The torture of a cigarette burn and the sensory confusion of hospital trips for every sniffle.
- The tainted joy of a laughing Mother after her first drink, the angst watching her knock back her tenth.
- The rage filled tears of being repeatedly ignored because you just don’t matter.
These are the extremes experienced by most children who ultimately are adopted.They are ugly and powered by deep raw emotion.They will not heal on their own, because these traumas, metaphoric infected wounds, are ‘picked at’ on a daily basis because the sensory triggers are all around.
In school just before lunch all the children in the class might be hungry. Only the child previously neglected will be running the unconscious programme “I really might die of hunger, because I remember when all I had to eat was mouldy bread and lumpy milk”. His desperate behaviour viewed by the teacher might seem very odd and interpreted as disruptive.
A traumatised child might find cigarette smoke or the smell of alcohol unbearable or deeply desirable – because of the internal feeling it triggers. During adolescence this has repercussions.
Measuring the damage of a traumatic experience
Metaphors can be a wonderful way for an audience to connect with a subject. So a number of years ago, when preparing a conference speech I devised a simple theoretical formula for quantifying the damage resulting from a traumatic event. My aim was to show how appropriate therapeutic input at an early stage can do much to reduce angst later.
Even though this is a model and isn't an assessment tool, some people have found it useful to "quantify the unquantifiable" to sense the scale of a child's traumatic experiences. If the word "formula" makes you shudder and reminds of you of disastrous maths lessons, then think of this as a recipe, (and notice how that old unpleasant event and memory from your school days impacts you and your level of functioning now, today....see the link...we all have triggers!!).
The component or ingredients include:
- INTENSITY of event - the severity of the event. E.g. a scratched knee, a nasty cut or bone poking through the skin.
- DURATION of event - how long did the event last? A moment, five minutes, an hour, a day, a fortnight?
- TIME TO RESOLUTION - how long before help and relief arrived? E.g. immediately, soon after, months later, years later or not yet.
- AGE AT TIME OF TRAUMA - the younger the age the more significant. The loss of a parent, or four months in hospital, is more damaging at three than at 30.
Most "normal everyday traumas" such as a grazed knee are resolved quickly. The little child who falls over in the playground and grazes his knee will maybe require an adult to wipe it, kiss it better, put on a plaster, etc. A seven year old may need reassurance the graze is clean and okay. The 14 year old will probably dismiss it, while the crawling baby will howl, need lots of cuddles and reassurances to calm and resolve the event. If the crawling baby's cries and sobs are ignored....then the damage is much greater.
There are a multitude of factors that make you 'you', which are not in the formula. These would include intelligence, resilience, learning style, personality, genetic inheritance, brain formation...and many, many more.
If you imagine a single unit of damage being a drop of liquid, then as the intensity and/or duration of the event increases the quantity of liquid increases. Some tiny little droplets, with explanations, reflection and maturity might evaporate. Others won’t.
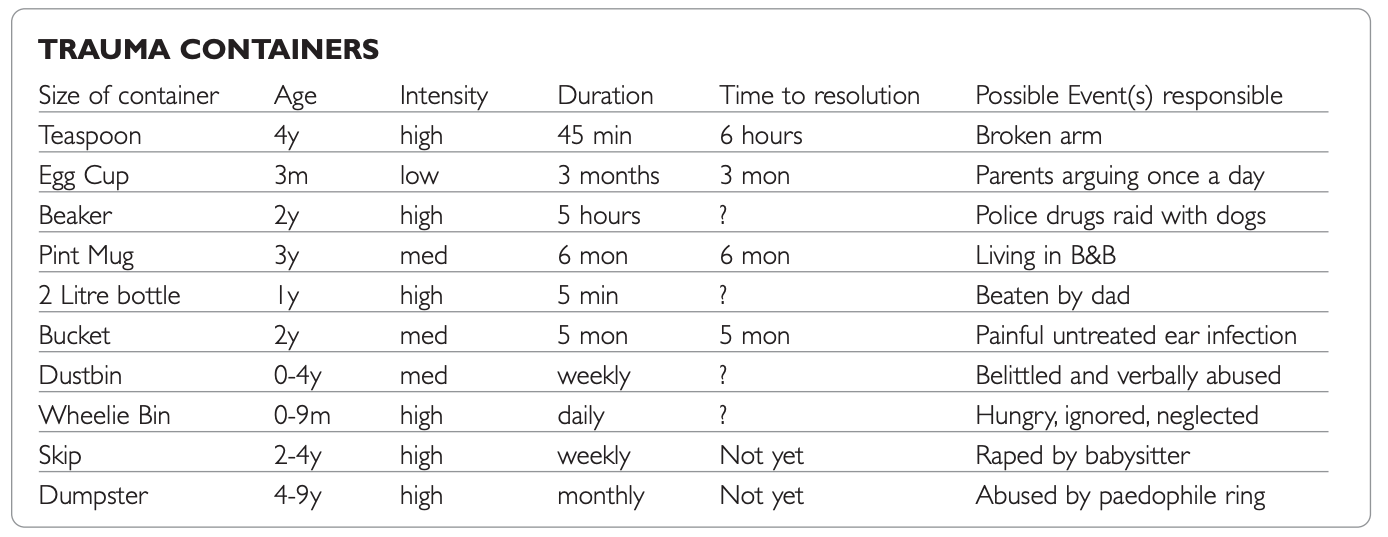
The following unscientific, invented scale of “Trauma Containers” illustrates the concept.
If a child had say a pint mug of trauma from the unsettling experience of living in a Bed and Breakfast, the volume might not increase if the situation was resolved and the child felt safe. It would probably stay pint sized.
The two-litre bottle of trauma from being beaten by Dad has not been resolved: the daughter cant make sense of the experience, so her inner rage increases daily. Aged 13 it may have grown to a gallon.
Managing and balancing the damage
Children find ways to hold the damage and still “function”.They find strategies and techniques to live with the hurt (maybe bizarre chameleon behaviour, stealing, ultra compliant, lying, aggression, self sabotaging antics etc).
It’s as if they counteract the damage with compensatory repairs. For every container of damage in the left hand there is a corresponding container of compensation in the right fist so they stay “balanced”. As they get older the unresolved trauma container gets bigger and bigger, so the compensatory strategies must increase.
Sometimes traumatised children can hold it together until they hit puberty.Then . . . KERPOW . . . a new shocking understanding about their childhood horrors combined with raging hormones wreak havoc with their identity, sense of self and how they interface with the world. Often they fall apart and/or explode. It’s not pretty and there is much collateral damage.
Unresolved trauma will fester, grow, magnify, distort, warp and maim the child . . . who as an adult might resort to drugs, alcohol, violence, depression, an anxiety disorder, obsessiveness, self harming, etc just to survive. I see this distorted view of self and lack of identity in many of my adult coaching clients.Trauma doesn’t just go away or heal on its own.
That’s why therapeutic reparenting and therapy which fully addresses Developmental Trauma disorder is essential for adopted children. (See Cost of Trauma article, Adoption Today, April 2008 for more detail). It’s not an optional extra; it is essential.
Afterthoughts
What if the “Trauma Container” chart below represented one child?
What if your child had six or more of the listed Trauma Containers when he arrived? How would you know? What would you do?
How many containers is your child clutching? What is their content? When will each unresolved trauma explode?
Can you afford to ignore the present behaviour and simply "hope it will go away"?
Take good care.
Helen x
This article was first published in Adoption Today in June 2008 - download here.
Never miss a post!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
